English
English
8:24 a.m.
Patient arrived in ED
A 67-year-old male with a history of arthritis presents with a chief complaint: severe pain that radiates from his left hip down to his knee — worse than his chronic arthritic pain.
The night prior, the patient had an acute onset of his pain when he tried to get up from his recliner. The pain worsened and the patient was taken to the ED the following morning.
8:29 a.m.
Initial Assessment: Tachycardia and limited range of motion of left hip due to pain.
The vitals assessed were normal except for an elevated pulse rate of 122 BPM, which was potentially attributed to the patient's pain.
T: 37.8 | BP: 114/59 | P: 122 | RR: 18 | SpO2: 98% (RA)
Considering the patient's age and exhibited tachycardia, complete blood count (CBC) differential and basic metabolic panel (BMP) labs were ordered.
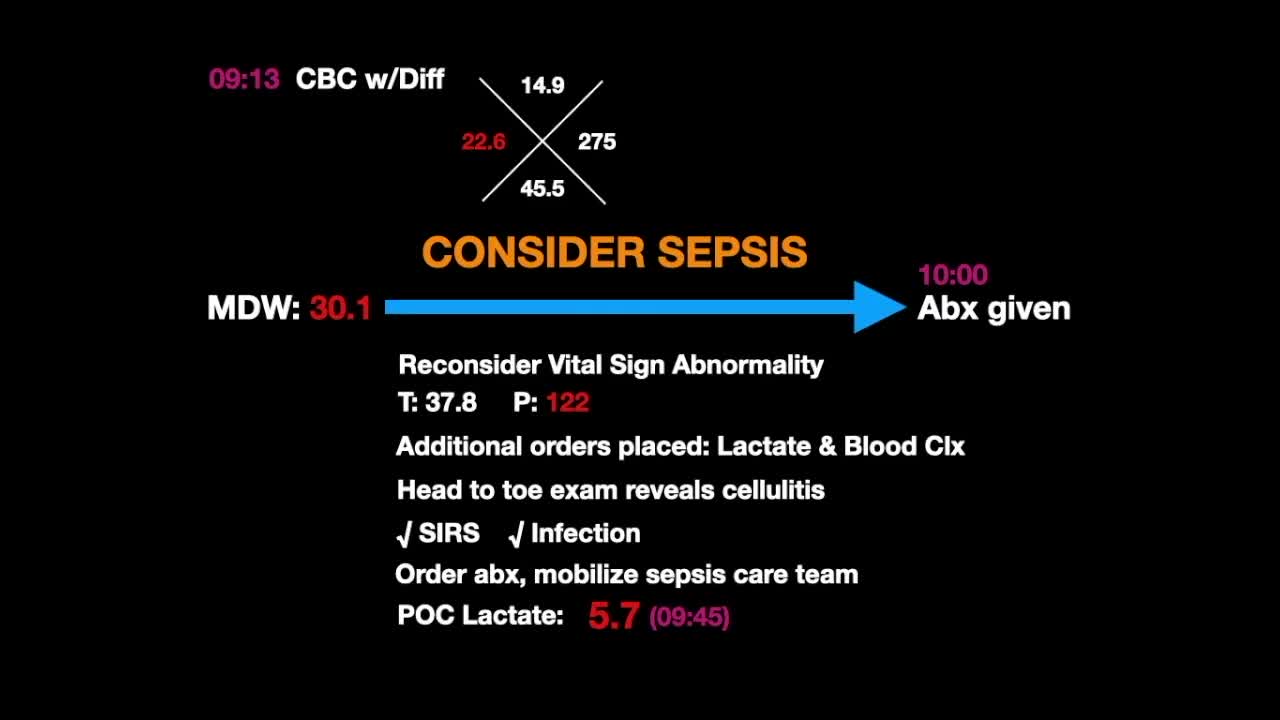
9:13 a.m.
CBC with Differential is Returned from the Lab: severe infection and risk of sepsis added to differential diagnosis.
The white blood cell (WBC) results come back elevated at 22.6, which could be attributed to the vomiting and stress due to significant pain. The monocyte distribution width (MDW) results come back at 30.1.
Due to the abnormal WBC and MDW results, the physicians deduced there might be an underlying infectious etiology. Reconsidering the vital signs abnormality, temperature of 37.8°C and elevated pulse rate of 122 BPM, lactate and blood cultures were ordered.
9:18 a.m.
Head to Toe Exam Reveals Erythema
With no skin changes, ecchymosis, bruising or swelling to the left extremities where the patient felt pain, the doctors were left pondering what they may be missing.
After a comprehensive exam, it was revealed that there was significant erythema of the right lower extremity that was tender and warm to palpation – this was suggestive of cellulitis.